Stem cells are unspecialized cells defined by two jobs: they can make more of themselves and they can turn into specialized cells. In the body, that lets them support growth, replace worn-out cells, and help repair some tissues after injury. In medicine, the same biology supports blood stem cell transplantation today and several newer cell-based approaches that are still being tested with care.[a][g]
A Clear Starting Point
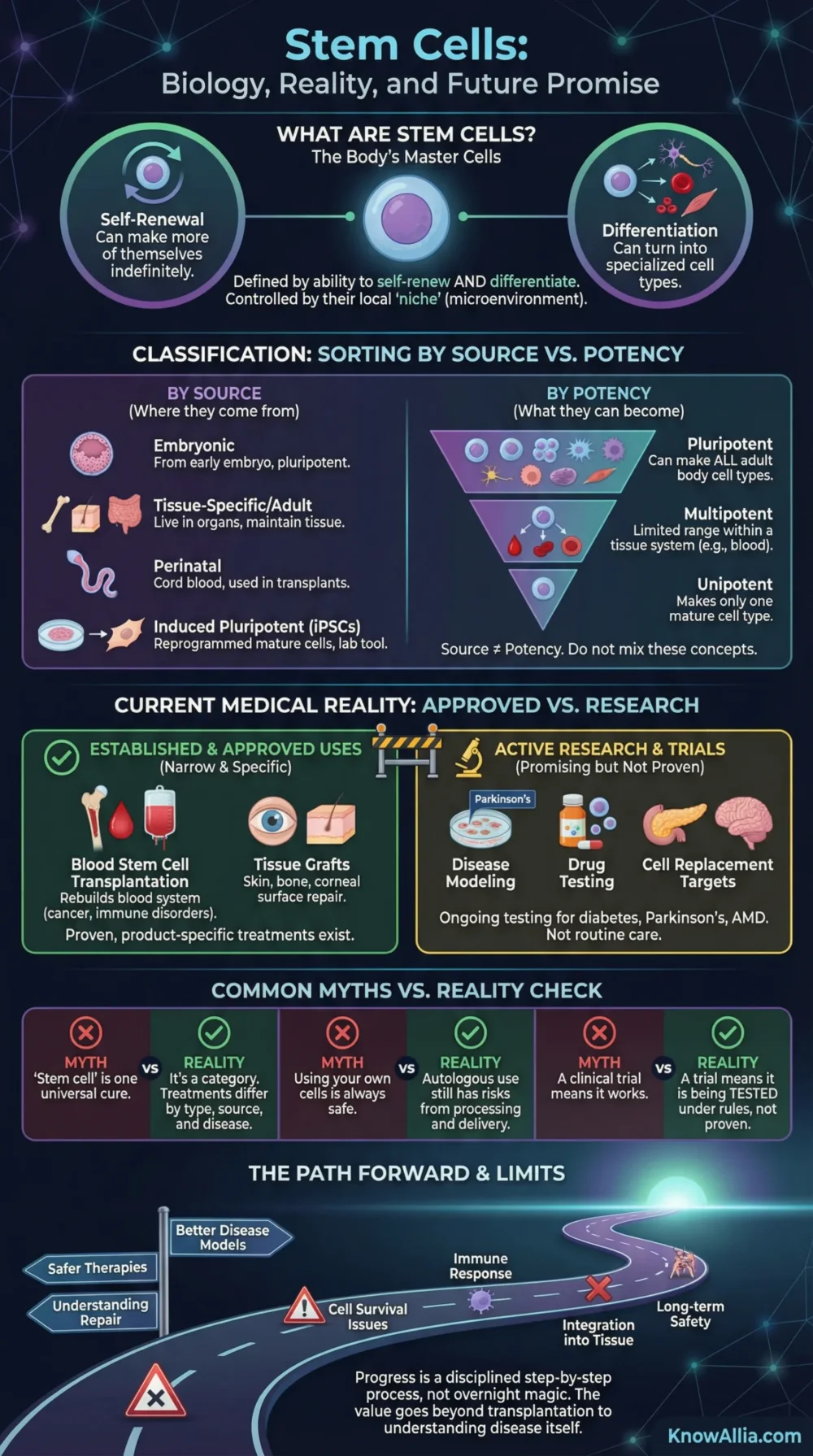
Stem cells matter because they sit at the meeting point of biology and medicine. They keep tissues running, they help scientists model disease in the lab, and in a few settings they already support approved care. The hard part is that not every stem cell can do every job, and not every treatment sold with the word “stem cell” has been proven.
- There are two separate ways to sort stem cells: by where they come from and by what they can become.
- Established medical use is still narrow and disease-specific, with blood stem cell transplantation as the clearest example.
- The most exciting near-term gains may come not only from transplantation, but also from disease modeling, drug testing, and better-targeted cell products.
This article explains the main types of stem cells, what they do inside the body, where they already help patients, why some newer ideas are promising, and where the limits are still real.
Contents
What Stem Cells Are
The two defining features are self-renewal and differentiation. Self-renewal means a stem cell can keep producing new stem cells. Differentiation means it can give rise to more specialized cells, such as blood cells, nerve cells, or muscle cells, depending on the stem cell type and the signals around it.[a][b]
- Self-Renewal
- Differentiation
- Potency
- Quiescence
- Niche Control
That does not mean stem cells are blank checks. Their behavior is tightly limited by biology. A blood-forming stem cell is excellent at making blood, but it does not naturally switch into a liver or brain cell inside the body. In practice, the phrase “stem cell” describes a class of cells with shared rules, not a universal repair tool.[a][g]
How They Are Sorted
One of the biggest sources of confusion is that stem cells are usually sorted in two different ways. Some labels describe origin. Others describe range. When those systems are mixed together, articles sound simpler than the science really is.
| Sorting Method | Typical Labels | What the Label Answers | Why It Matters |
|---|---|---|---|
| By source | Embryonic, tissue-specific/adult, perinatal, induced pluripotent | Where the cells come from or how they were made | Useful when discussing collection, lab handling, and clinical use |
| By potency | Totipotent, pluripotent, multipotent, unipotent | How wide a range of cell types the cell can make | Useful when discussing biological limits and therapeutic fit |
Types by Source
- Embryonic stem cells come from the inner cell mass of a very early embryo and are pluripotent, meaning they can form all cell types of the adult body.[a][g]
- Tissue-specific stem cells, often called adult stem cells, live in organs and tissues. They usually maintain the tissue where they reside, such as bone marrow, skin, gut lining, or the corneal edge of the eye.[a][j]
- Perinatal sources, especially umbilical cord blood, are important in real-world medicine because they can provide blood-forming cells for transplant.[c][d]
- Induced pluripotent stem cells, or iPSCs, are made by reprogramming mature cells, such as skin or blood cells, back into a pluripotent state. That makes them valuable for lab research, disease models, drug testing, and candidate cell therapies.[a][i]
Potency in Plain Language
- Totipotent cells can generate both the body itself and the extra tissues needed very early in development. In humans, this term belongs to the earliest embryonic stages, not to routine clinical cells.[b]
- Pluripotent cells can generate any cell type in the adult body, but not the extra embryonic support tissues.[a]
- Multipotent cells can generate several related cell types inside one tissue system, such as the many mature blood cells produced by hematopoietic stem cells.[b][j]
- Unipotent cells sit near the edge of stem cell terminology. They can renew themselves but usually make only one mature cell type.[b]
A practical rule helps here: source tells you where a cell came from; potency tells you how much range it has. Those are different questions, and good explanations keep them separate.
What They Do in the Body
Inside living tissue, stem cells are less visible than the cells they replace. Many stay quiet for long periods, then wake up when normal turnover, stress, or injury creates demand. This is one reason tissues with heavy daily wear, such as blood, skin, and the lining of the gut, depend so much on them.[a][g]
Their behavior is controlled by the stem cell niche, the local microenvironment around them. If the stem cell is the seed, the niche is the soil: neighboring cells, extracellular matrix, blood supply, and chemical signals help decide whether the cell stays quiet, copies itself, or begins to specialize.[j][a]
Another useful distinction is the one between a stem cell and a progenitor cell. Progenitors usually come after stem cells in the line of development. They can divide quickly and are very useful for tissue production, but they tend to have a narrower fate and less staying power over time. That difference matters in research, because a cell that looks regenerative at first glance may not have the long-term behavior of a true stem cell.[b][j]
Where They Already Help Patients
The present-day medical picture is more focused than many headlines suggest. Approved use exists, but it is narrow, product-specific, and tied to particular diseases and delivery methods. There is no single stem cell treatment that works across unrelated conditions.[l][d]
- Blood stem cell transplantation is the clearest established example. It is used to rebuild the blood system after intensive treatment and to treat some blood cancers, blood disorders, and immune disorders. Depending on the case, cells may come from bone marrow, peripheral blood, or cord blood.[c]
- Tissue grafts that rely on resident stem cells are another real-world use. Some skin, bone, and corneal procedures work in part because the transplanted tissue carries cells that can keep renewing the treated surface.[l]
- Corneal surface repair has moved further than many readers expect. In the European Union, Holoclar is authorized for certain adults with moderate to severe limbal stem cell deficiency caused by eye burns.[f]
- Newer cell products can be real without being broad. In the United States, the FDA approved Ryoncil in 2024 for pediatric steroid-refractory acute graft-versus-host disease after donor blood stem cell transplant. That is a narrow indication, not proof that products marketed for many unrelated problems are ready for routine care.[e][d]
One point is easy to miss: regulatory status depends on the exact product, the disease being treated, the route of delivery, and the evidence behind it. A real approval in one setting does not validate other uses built around similar words or similar cells.[d][l]
Why the Medical Promise Is Real
The promise of stem cell science is not only about transplanting cells into patients. A large share of its value comes from understanding disease, testing drugs, and learning how tissues fail and recover. Patient-derived iPSCs are especially useful because researchers can turn them into disease-relevant cells in the lab and study problems that are otherwise hard to reach, such as neurons or heart muscle cells.[i]
- Disease modeling: building lab models that reflect human disease biology more closely than many older systems.[i]
- Drug discovery and safety testing: checking how candidate therapies affect human cell types before later clinical steps.[i]
- Cell replacement: creating carefully defined cells to replace tissue lost in disease or injury.[i][h]
- Endogenous repair: finding ways to help the body’s own repair systems work better instead of adding outside cells.[i]
Several areas remain active targets for cell-based trials, including type 1 diabetes, Parkinson’s disease, and age-related macular degeneration. What matters most is the wording: these are areas of active testing, not blanket proof that the treatments already work in everyday care.[l][h]
The eye offers a good example of how the field moves. Corneal work is already helping some patients in carefully defined settings, while related eye programs are still moving through trial stages. The difference is not hype versus failure. It is the normal pace of clinical translation, where each cell type, tissue target, dose, and delivery method has to earn its place step by step.[f][k][h]
How Stem Cells Move From Biology to Care
The path is rarely direct. A cell type may look useful in the lab, then face harder questions about identity, delivery, long-term function, and safety before it reaches everyday medicine.
Typical Development Path
Source Cells Embryonic, tissue-specific, cord blood, or iPSC-derived Cell Identity Purity, potency, stability, and manufacturing control Preclinical Work Dose, delivery route, tumor risk, off-target effects Clinical Trials Safety first, then benefit, then longer follow-up Approved Use Only for the setting that matched the evidence Already in Regular Care Blood stem cell transplantation and selected eye-surface or tissue-based regenerative procedures Active Research Targets Beta cells, retinal support cells, dopamine neurons, immune-modulating products, organoid-based testing What Usually Slows Progress Cell survival, tissue integration, immune response, durability, manufacturing consistency, late effectsThe same cell label does not make two products equivalent. Source, processing, dose, and delivery all change the clinical meaning.
A wider developmental range can be useful in the lab, but fit, control, and safety matter just as much in patients.
A good trial asks whether one defined product helps one defined group under one defined protocol.
Today’s Clearest Clinical Role
Replacing or restoring blood-forming cells remains the strongest day-to-day example of stem-cell-based medicine.
Fast-Moving Research Space
iPSC-derived models are making it easier to test human disease biology and drug responses with cell types once hard to study.
What Makes the Field Valuable
Its value is broader than transplantation alone: it changes how researchers study disease, screen therapies, and think about tissue repair.
Common Confusion
Terms Worth Knowing
- Self-Renewal
- The ability of a stem cell to make more stem cells over time.
- Differentiation
- The process by which a less specialized cell becomes a more specialized one.
- Potency
- The range of cell types a stem cell can generate.
- Niche
- The local microenvironment that regulates whether stem cells stay quiet, divide, or specialize.
- Progenitor Cell
- A descendant of a stem cell with a narrower fate and usually shorter renewal capacity.
- Autologous
- Cells taken from and used in the same person.
- Allogeneic
- Cells taken from one person and used in another.
- Engraftment
- The point at which transplanted cells take hold and begin functioning in the recipient.
- Organoid
- A lab-grown three-dimensional model made from stem cells that mimics parts of an organ.
What Is Not Settled Yet
Stem cell science is moving, but some questions are still open. Researchers are still sorting out which cell type is best for which disease, what dose and delivery route work best, how long transplanted cells remain useful, how to reduce immune and safety problems, and when benefit comes from true cell replacement versus cell-to-cell signaling.[h][i]
- Some tissues are easier to rebuild than others.
- Making the right cell is only part of the job; the cell must also survive, integrate, and behave predictably.
- Long follow-up matters, because late effects can be just as important as short-term benefit.
- Careful trials remain the only reliable way to separate real benefit from hopeful interpretation.
That is why the field advances one product, one disease, and one trial at a time. The real story is not slower than readers want. It is more disciplined than marketing language tends to be.
FAQ
What is the difference between a stem cell and a progenitor cell?
A stem cell can renew itself for long periods and can produce more specialized descendants. A progenitor cell usually comes later in the lineage, has a narrower fate, and has less long-term renewal capacity.
Are all stem cells pluripotent?
No. Pluripotent stem cells can make any cell type in the adult body, but many stem cells in ordinary tissues are multipotent and stay within the needs of their own organ or system.
Which stem cell treatments are already used in regular care?
The clearest established example is hematopoietic stem cell transplantation for selected blood, immune, and bone marrow conditions. Some eye-surface and tissue-based regenerative procedures also rely on tissue-specific stem cells in defined settings.
Does using your own cells make a stem cell treatment proven?
No. Autologous treatment may change some immune questions, but it does not prove that the product is well characterized, effective, or safe for the condition being treated.
Why are induced pluripotent stem cells such a big deal?
They let researchers make pluripotent cells from mature cells such as skin or blood. That has made disease modeling, drug testing, and patient-specific research much easier.
Do stem cells always repair damaged tissue after they are injected?
No. Some cells fail to survive, fail to integrate, or do not produce a useful effect. In some settings, any benefit may come more from signaling and immune effects than from direct tissue replacement.
Sources
- [a] NIH – Stem Cell Basics — definition, self-renewal, pluripotent versus adult stem cells.
- [b] NCBI Bookshelf – Basics of Stem Cell Biology as Applied to the Brain — potency terms and the stem cell–progenitor distinction.
- [c] National Cancer Institute – Stem Cell and Bone Marrow Transplants for Cancer — how hematopoietic stem cell transplant works and where it is used.
- [d] U.S. Food and Drug Administration – Consumer Alert on Regenerative Medicine Products Including Stem Cells and Exosomes — product-specific approval and caution around unapproved interventions.
- [e] U.S. Food and Drug Administration – FDA Approves First Mesenchymal Stromal Cell Therapy to Treat Steroid-refractory Acute Graft-versus-host Disease — the 2024 Ryoncil approval and its narrow indication.
- [f] European Medicines Agency – Holoclar — limbal stem cell therapy authorized in the European Union for certain eye-burn cases.
- [g] About Stem Cells / ISSCR – Types of Stem Cells — source-based types and why tissue-specific stem cells are more limited than pluripotent cells.
- [h] About Stem Cells / ISSCR – Clinical Translation — why the path from lab findings to approved treatment takes years and often ends in failure.
- [i] About Stem Cells / ISSCR – Stem Cell Research — disease modeling, drug testing, endogenous repair, and cell replacement.
- [j] EuroGCT – Blood Stem Cells: The Pioneers of Stem Cell Research — blood stem cells, their niche, and their role in normal blood production.
- [k] National Eye Institute – Novel Stem Cell Therapy Repairs Irreversible Corneal Damage in Clinical Trial — a current eye-surface example that is promising but still in the trial stage.
- [l] About Stem Cells / ISSCR – Types of Stem Cell Treatments — approved uses, active trial areas, and the difference between established and investigational treatment.